Ever since the Supreme Court struck down Roe v. Wade, in the Dobbs decision, pro-abortion liberals have been pretending that abortion is unavailable in the U.S. In truth, there is no evidence the number of abortions has declined. In fact, the evidence is to the contrary.
The Guttmacher Institute recently released data showing in the first 10 months of 2023, there were an estimated 878,000 abortions in the U.S. health care system, 94% as many abortions as were provided in 2020 (930,000). At that rate, 2023 would easily eclipse the number of abortions done in 2020.
They state “The actual increase in abortions is likely even larger than these numbers suggest because these counts do not include abortions occurring outside the formal health care system, which are likely to have increased substantially following the implementation of state bans and restrictions.”
They go on to say many factors have contributed to more abortions in 2023, including the following:
- Abortions were already increasing in many US states prior to theDobbs decision, as reported in Guttmacher’s 2020 Abortion Provider Census: Abortions increased by 8% from 2017 to 2020, reversing 30 years of a declining abortion rate.
- Interstate travel for abortion care has increased, largely facilitated by practical support networks(like abortion funds) that have helped patients navigate financial and logistical barriers.
- Access to abortion has increased instates that passed protective abortion policies following the fall of Roe v. Wade.
- Abortion provided via telehealth has become increasingly available.
All this information from an institute that promotes abortion.
Which begs the question, why are liberals lying about the availability of abortion? The most recent propaganda is the U.S. has a “pregnancy crisis” due to supposedly soaring maternal mortality, not to declining fertility.
Allysia Finley, writing for The Wall Street Journal, reports that the American Medical Association claims the U.S. stands out among high-income nations for its alarming incidence of maternal deaths despite substantial health care spending. These liberal activists invoke U.S. maternal mortality to advocate expanded government welfare programs and abortion access.
“Evidence and experience show us conclusively that the risk of death during or after childbirth is approximately 14 times greater than the risk of death from abortion-related complications,” the AMA says. Democratic states echo this claim in a friend-of-the-court brief in FDA v. Alliance for Hippocratic Medicine, which the Supreme Court will hear Tuesday. Justices who were about to overturn Roe v. Wade would have “blood on their hands,” the medical journal Lancet warned in a May 12, 2022, editorial.
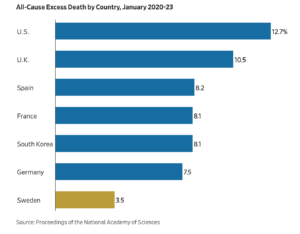
Finley explains, as with the Covid pandemic, experts are using bad data to drive a political agenda. A new study this month in the American Journal of Obstetrics and Gynecology shows that oft-cited U.S. maternal-mortality statistics are inflated owing to discrepancies in how pregnancy deaths are recorded.
The Centers for Disease Control and Prevention’s National Vital Statistics System reports that maternal-mortality rates in the U.S. have roughly tripled since 2001, to 32.9 per 100,000 live births in 2021. This is nearly three times as high as rates in other developed countries—but, as the study concludes, it’s largely a statistical artifact.
Deaths among pregnant women or new mothers are often classified as “maternal” even if they owe to other causes, such as cancer or pre-existing conditions. The culprit is a check box that states added to death certificates in 2003 to identify women who had died while pregnant or between 42 days and a year of when their pregnancy ended.
As the study explains, this check box “led to a rapid increase in reported maternal mortality rates” and “some egregious errors,” including hundreds of women over 70 “being certified as pregnant at the time of death or in the year before death” largely because of administrative errors.
Researchers reanalyzed mortality data to identify only deaths that occurred during pregnancy or postpartum that had at least one mention of pregnancy among the causes of death on the certificate. The authors found that the maternal mortality rate remained essentially flat between 1999 and 2002 (10.2 per 100,000 live births) and 2018 and 2021 (10.4). This would put the U.S. on par with other developed countries.
Lest you think the AMA is a credible source of information, you should know that only about 12% of all U.S. physicians are members of the AMA. Personally, I dropped my AMA membership about 30 years ago as soon as I realized they were promoting abortion back then. It seems nothing has changed since then.